Adrenal incidentaloma (AI) refers to adrenal tumors with a diameter ≥1 cm that are incidentally discovered during imaging studies conducted for health screening or unrelated conditions, excluding adrenal diseases explicitly indicated by patient history or physical examination. Common findings include benign adrenal cortical tumors, with less common occurrences such as adrenal metastases, adrenal cortical carcinoma, adrenal cysts, adrenal hematomas, myelolipomas, and teratomas.
To determine the origin and nature of these tumors, it is recommended to assess for malignancy upon initial detection and conduct laboratory tests to evaluate adrenal function.
Imaging Studies
Ultrasound Examination
This is typically used as an initial screening tool.
Adrenal CT
For tumors with a diameter <4 cm, the malignancy rate is below 2%. Most adrenal cortical carcinomas have a diameter >6 cm, and adrenal metastases are more commonly observed than primary adrenal cortical carcinoma. Solid adrenal masses with a diameter >6 cm should be considered potentially malignant prior to surgical resection.
MRI Examination (Optional)
This can evaluate the presence of fat using in-phase and out-of-phase imaging and is suitable for pregnant women, children, or patients with contrast agent allergies.
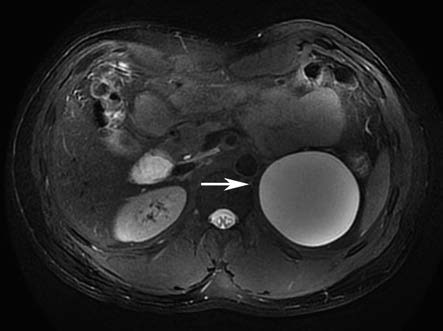
Figure 1 MRI of left adrenal cyst
PET-CT (Optional)
This is generally reserved for cases where CT findings are inconclusive or for patients with a history of malignant tumors.
Assessment of Endocrine Function
A comprehensive evaluation of clinical symptoms, signs, and laboratory tests is recommended for all patients with incidentalomas to determine the presence of catecholamine excess, cortisol excess, primary aldosteronism, or abnormalities in sex hormones. Confirmatory testing is indicated for patients with suspicious screening results.
Treatment
Non-Surgical Management:
For asymptomatic, non-functioning unilateral incidentalomas with a diameter <3 cm that are confirmed as benign by imaging, surgical treatment is not recommended.
Surgical Treatment:
Surgical intervention may be considered for tumors with hormone secretion, imaging features suggestive of malignancy, isolated adrenal metastases, or tumors with rapid growth or an increase in size exceeding 20%. For tumors with a diameter ≥3 cm that are considered benign based on imaging and are non-functional, the decision to proceed with surgery should take into account the patient’s overall health status and personal preference.
Surgical Approaches
Laparoscopic Surgery
The preferred approach for adrenal tumor resection due to its minimal invasiveness and faster recovery. For larger tumors, robotic-assisted laparoscopic surgery may also be considered.
Open Surgery
This is indicated for tumors with a diameter ≥6 cm, or for metastatic tumors and adrenal cortical carcinomas with evidence of invasion into surrounding tissues.