Anterior urethral injuries in males most commonly occur in the bulbar urethra. These injuries are often caused by straddle injuries to the perineum, which compress the urethra against the pubic symphysis, leading to bulbar urethral damage. Repeated catheterizations and urethral manipulations may also result in anterior urethral injuries.
Pathology
Anterior urethral injuries can be classified into contusions, lacerations, and ruptures.
Contusion
Contusion involves localized edema and bleeding, with healing typically not leading to urethral stricture.
Laceration
In lacerations, a portion of the urethral wall remains intact, but healing often results in scar-related urethral stricture.
Rupture
Complete rupture entails total separation of the urethra, with the ends retracting and becoming disconnected. In cases of bulbar laceration or rupture, blood and urine may extravasate into the superficial perineal pouch enveloped by the superficial perineal fascia, causing swelling in the perineum, scrotum, or penis. In some cases, extravasation extends upward to the abdominal wall. The distal attachment of the superficial perineal fascia at the inguinal region and its proximal connection to the deep layer of the abdominal wall fascia prevent urine from extravasating into the thighs.
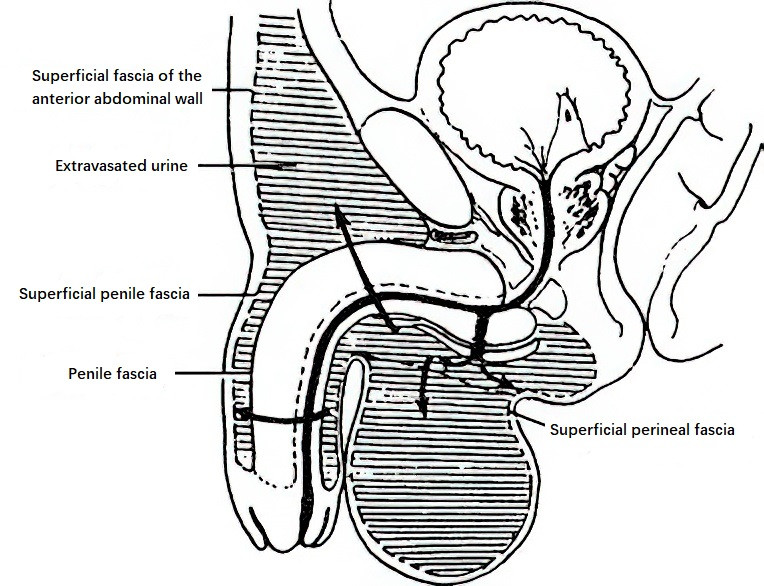
Figure 1 Extravasation range in urethral bulb rupture
For injuries to the penile urethra, if the penile fascia remains intact, urine and blood extravasation are confined within the fascia, presenting as penile swelling. However, if the fascia is disrupted, extravasation increases in scope and is similar to that observed in bulbar urethral injuries.
Clinical Manifestations
Urethral Bleeding
Bright red blood dripping from the external urethral meatus is the most common symptom of anterior urethral injury.
Pain
Localized pain and tenderness are common, often presenting with dysuria and radiating to the glans penis or perineum.
Localized Hematoma
Straddle injuries to the urethra may result in swelling, ecchymosis, or butterfly-shaped hematomas in the perineum or scrotum.
Difficulty Urinating
Urethral lacerations or ruptures may lead to dysuria or urinary retention.
Urine Extravasation
Urethral lacerations or ruptures may result in urine leaking into surrounding tissues. Improper management can lead to widespread subcutaneous tissue necrosis, infection, or even septicemia. Infections may result in perurethral abscess formation, and abscess rupture may lead to urethral fistula formation.
Diagnosis
Medical History and Physical Examination
Bulbar urethral injury is often associated with a history of perineal straddle trauma or urethral manipulations. The diagnosis can be established based on medical history, typical symptoms, and the distribution of hematoma or urine extravasation.
Diagnostic Catheterization
Catheterization provides information regarding urethral integrity and continuity. Successful catheterization on the first attempt suggests mild urethral injury, with the catheter retained for drainage and urethral support. Difficulty or failure during the first attempt indicates potential urethral laceration or rupture, and repeated attempts should be avoided to prevent further damage.
Retrograde Urethrography
Retrograde urethrography identifies the location and severity of the urethral injury. Contrast extravasation suggests partial laceration, while significant extravasation without entry into the posterior urethra suggests severe laceration or rupture of the anterior urethra.
Treatment
Emergency Management
Severe bleeding from the urethral bulbous spongiosum may lead to shock and requires immediate compression of the perineum to stop the bleeding and anti-shock measures. Patients with urinary retention may undergo suprapubic cystostomy for urinary drainage if catheterization fails.
Management of Urethral Contusion
Patients with intact urethral continuity typically do not require specialized treatment. Hemostasis and analgesia are provided, along with antibiotics to prevent infection. When necessary, a urinary catheter is retained for drainage for approximately one week.
Management of Urethral Laceration
When catheterization is successful, the catheter is retained for about two weeks. If catheterization fails, partial urethral laceration may be suspected. Immediate perineal urethral repair is performed, followed by catheterization for two to three weeks.
Management of Urethral Rupture
Complete rupture of the distal bulbar and penile urethra may result in significant hematoma formation in the perineum, penis, or scrotum. Timely exploration via perineal incision is required, followed by end-to-end urethral anastomosis, with catheterization maintained for three weeks.
Management of Complications
Urine Extravasation
Early management involves multiple incisions at the extravasation sites that extend below the superficial fascia for drainage with porous drainage tubes. Suprapubic cystostomy is also performed, and urethral repair is delayed for approximately three months.
Urethral Stricture
Urethral stricture is the most common late complication. In mild cases, regular urethral dilation suffices. For stricture at the external urethral meatus, meatal incision is performed. Severe strictures causing dysuria or a reduced urine stream may require internal urethrotomy using endoscopic cold knife techniques, with adjunctive electrosurgical or laser procedures for severe scarring. Severe cases resulting in urethral obstruction require perineal segment resection and end-to-end urethral anastomosis.
Urethral Fistula
Urethral fistulas secondary to anterior urethral strictures are commonly localized to the perineum or scrotum. Management involves addressing the stricture alongside excision or cleaning of the fistula tract.