Gallbladder cancer is the most common type of malignant tumor in the gallbladder. Other types of malignant tumors include lymphoma, rhabdomyosarcoma, carcinoid, and carcinosarcoma. The majority of cases occur in individuals aged 60–70, with an incidence in women approximately 2–3 times higher than in men. Gallbladder cancer accounts for only 0.4%–3.8% of biliary diseases but constitutes 25% of extrahepatic biliary cancers.
Etiology
Gallbladder cancer is seven times more likely to be associated with gallstones than with cases of gallbladder cancer without gallstones. Patients with gallstones larger than 3 cm have a tenfold higher risk of developing gallbladder cancer compared to those with gallstones under 1 cm, indicating a significant relationship between gallstones and gallbladder cancer. Gallstones may contribute to gallbladder cancer through prolonged physical irritation, combined with factors such as chronic inflammation of the mucosa and carcinogenic substances from bacterial products. Other conditions potentially associated with gallbladder cancer include cholecystoenteric anastomosis, the completely calcified "porcelain" gallbladder, gallbladder adenoma, bile and pancreatic ductal junction anomalies, and ulcerative colitis.
Pathology
Gallbladder cancer is typically classified into infiltrative, nodular, papillary, and mixed types. Approximately 90% of cases arise in the body or fundus of the gallbladder. Adenocarcinoma is the most common histological type, accounting for about 82% of cases, followed by undifferentiated carcinoma (7%), squamous cell carcinoma (3%), and mixed carcinoma (1%). Most gallbladder cancers grow in an infiltrative pattern, ultimately involving the entire gallbladder wall. Due to the thin muscular layer covered by a serosal membrane between the gallbladder and the liver at the gallbladder bed, these tumors can invade the liver directly at an early stage. Gallbladder cancer can also spread intrahepatically or systemically through venous reflux from the gallbladder. Lymphatic metastasis is common and often follows a pathway from the gallbladder lymph nodes to lymph nodes around the common bile duct, followed by the pancreatic head, peripancreatic, superior mesenteric, hepatic artery, and para-aortic lymph nodes. Direct invasion of nearby structures such as the duodenum, stomach, or transverse colon is also possible. Intraperitoneal seeding and metastasis can occur through the shedding of cancer cells into the abdominal cavity.
Staging
The American Joint Committee on Cancer (AJCC) TNM staging system is widely used for gallbladder cancer. This staging system is important for guiding treatment and predicting prognosis.
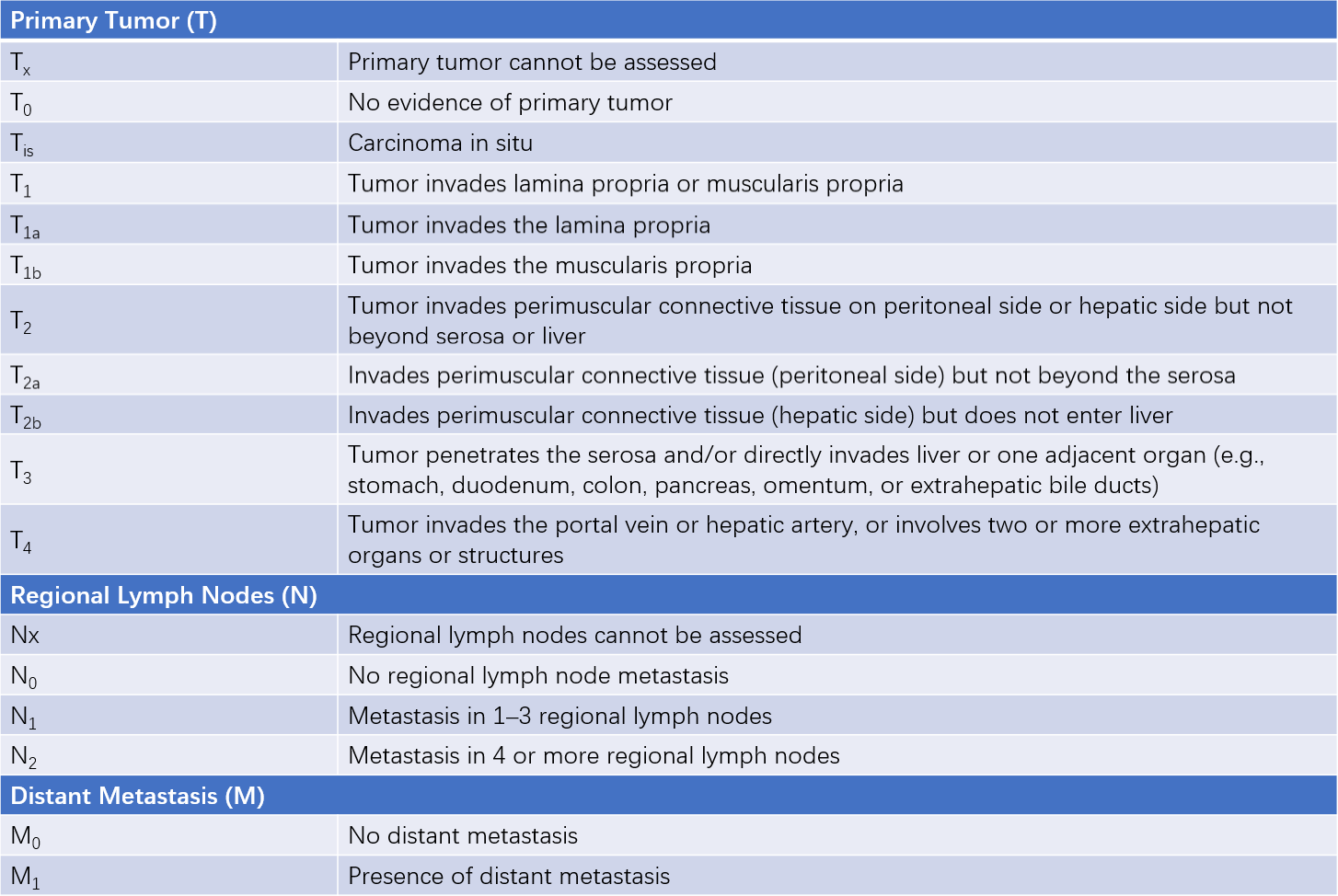
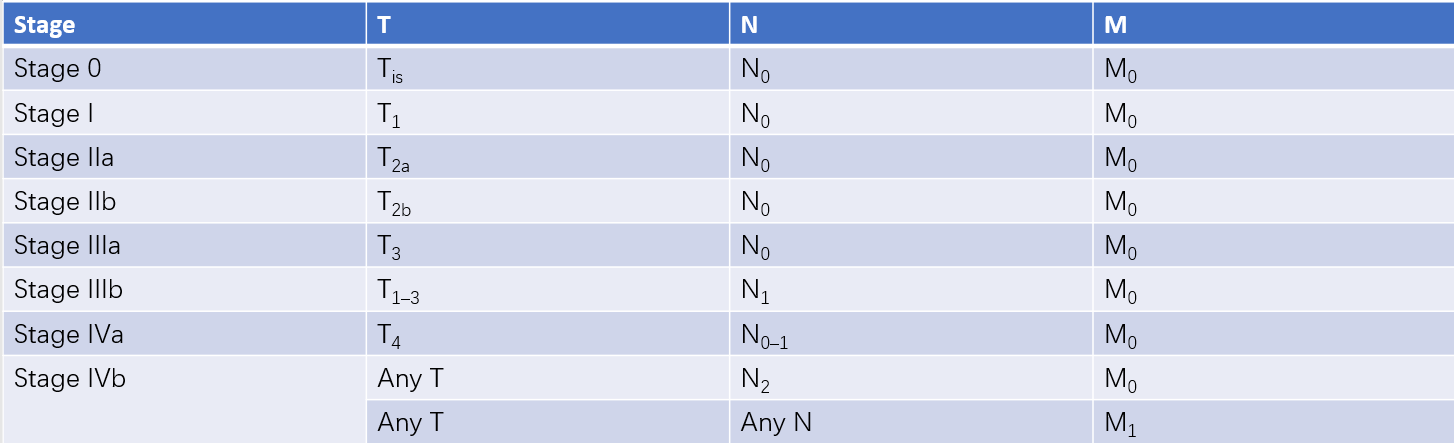
Figure 1 AJCC 8th edition TNM staging of gallbladder cancer
Clinical Features
Gallbladder cancer often presents without specific symptoms in the early stages. When diagnosed postoperatively following cholecystectomy performed for gallstones or other benign conditions, it is referred to as "unsuspected/unexpected gallbladder carcinoma" (UGC). Once the tumor invades the serosa or gallbladder bed, symptoms such as right upper abdominal pain radiating to the shoulder or back may occur. Obstruction of the cystic duct may lead to a palpable enlarged gallbladder. Symptoms such as abdominal distension, loss of appetite, weight loss, anemia, hepatomegaly, jaundice, and ascites suggest advanced disease. Perforation of the gallbladder due to tumor penetration of the serosa can cause peritonitis. Chronic perforation into the stomach or intestines may result in the formation of an internal fistula, which could lead to biliary bleeding.
Diagnosis and Differential Diagnosis
Laboratory Tests
Levels of tumor markers such as CEA, CA19-9, and CA125 may be elevated, with CA19-9 being the most sensitive, although none are specific to gallbladder cancer.
Imaging Studies
Ultrasound or CT imaging may reveal irregular thickening of the gallbladder wall and fixed, non-mobile mass lesions within the lumen, raising suspicion of gallbladder cancer. Findings from contrast-enhanced ultrasound, contrast-enhanced CT, or MRI showing hypervascularity in gallbladder masses further support the diagnosis of gallbladder cancer.
Differential Diagnosis
Gallbladder cancer with secondary infection or necrosis needs to be differentiated from complications of gallbladder inflammation or gangrenous cholecystitis forming an abscess. Gallbladder cancer is often distinguished by its hypervascularity and the elevation of CA19-9.
Treatment
The primary treatment for gallbladder cancer is surgical resection. The extent of surgical removal is determined based on the stage of the disease.
Simple Cholecystectomy
This procedure is suitable for AJCC stage 0 and stage I gallbladder cancer. In most cases, these cancers are incidentally identified during pathological examination after cholecystectomy performed for gallstones or cholecystitis. The tumor remains confined to the mucosa or muscularis propria and does not invade deeper layers, making further surgery unnecessary.
Radical Cholecystectomy
Radical resection is indicated for stage IIa, IIb, and IIIa gallbladder cancer. In addition to removing the gallbladder, this operation involves resection of liver segments IVb (quadrate lobe) and V or subhepatic segments, as well as regional lymph node dissection in the area of gallbladder drainage.
Extended Radical Cholecystectomy
This is performed in cases involving advanced-stage gallbladder cancer, such as select stage IIIb, IVa, or IVb tumors. The surgical scope may include resection of the right tri-segment of the liver and, in some cases, combined liver and pancreaticoduodenectomy.
Palliative Surgery
For unresectable gallbladder cancer, palliative procedures may be undertaken. These can include hepaticojejunostomy with Roux-en-Y anastomosis for internal drainage of bile, placement of percutaneous transhepatic or endoscopic biliary stents at the site of bile duct obstruction, or gastrojejunostomy. The aim of these procedures is to alleviate or resolve jaundice or duodenal obstruction caused by the tumor.
Adjuvant Therapy
For advanced stages, chemotherapy regimens based on gemcitabine, often combined with platinum-based agents, are commonly used. Some case reports also highlight the effectiveness of immunotherapy in combination with targeted therapies.
Prevention
The long-term survival rate following surgery for gallbladder cancer remains low. Prophylactic cholecystectomy in patients with symptomatic gallstones, especially when the stones are larger than 3 cm, is considered beneficial in reducing the risk of gallbladder cancer. Similarly, solitary gallbladder polyps larger than 1 cm in diameter or with broad bases, adenomatous polyps, and a "porcelain" gallbladder may warrant proactive removal of the gallbladder to prevent cancer development.